The choice of treatment depends mainly on the location of the tumor in the colon or rectum and the stage of the disease.
Treatment for colorectal cancer may involve surgery, chemotherapy, biological therapy or radiation therapy. Some people have a combination of treatments. These treatments are described below.
Colon cancer sometimes is treated differently from rectal cancer. Treatments for colon and rectal cancer are described separately below.
Your doctor can describe your treatment choices and the expected results. You and your doctor can work together to develop a treatment plan that meets your needs.
Cancer treatment is either local therapy or systemic therapy:
- Local therapy: Surgery and radiation therapy are local therapies. They remove or destroy cancer in or near the colon or rectum. When colorectal cancer has spread to other parts of the body, local therapy may be used to control the disease in those specific areas.
- Systemic therapy: Chemotherapy and biological therapy are systemic therapies. The drugs enter the bloodstream and destroy or control cancer throughout the body.
Because cancer treatments often damage healthy cells and tissues, side effects are common. Side effects depend mainly on the type and extent of the treatment. Side effects may not be the same for each person, and they may change from one treatment session to the next. Before treatment starts, your health care team will explain possible side effects and suggest ways to help you manage them.
Surgery
Surgery is the most common treatment for colorectal cancer.
- Colonoscopy: A small malignant polyp may be removed from your colon or upper rectum with a colonoscope. Some small tumors in the lower rectum can be removed through your anus without a colonoscope.
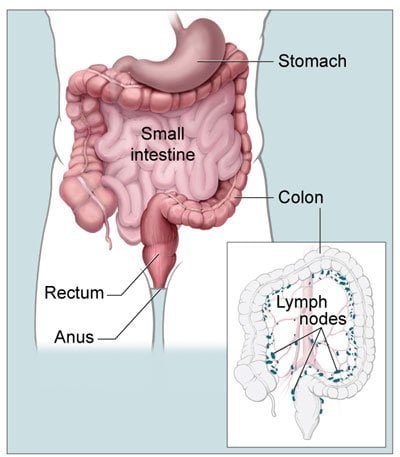
- Laparoscopy: Early colon cancer may be removed with the aid of a thin, lighted tube (laparoscope). Three or four tiny cuts are made into your abdomen. The surgeon sees inside your abdomen with the laparoscope. The tumor and part of the healthy colon are removed. Nearby lymph nodes also may be removed. The surgeon checks the rest of your intestine and your liver to see if the cancer has spread.
- Open surgery: The surgeon makes a large cut into your abdomen to remove the tumor and part of the healthy colon or rectum. Some nearby lymph nodes are also removed. The surgeon checks the rest of your intestine and your liver to see if the cancer has spread.
When a section of your colon or rectum is removed, the surgeon can usually reconnect the healthy parts. However, sometimes reconnection is not possible. In this case, the surgeon creates a new path for waste to leave your body. The surgeon makes an opening (stoma) in the wall of the abdomen, connects the upper end of the intestine to the stoma, and closes the other end. The operation to create the stoma is called a colostomy. A flat bag fits over the stoma to collect waste, and a special adhesive holds it in place.
For most people, the stoma is temporary. It is needed only until the colon or rectum heals from surgery. After healing takes place, the surgeon reconnects the parts of the intestine and closes the stoma. Some people, especially those with a tumor in the lower rectum, need a permanent stoma.
People who have a colostomy may have irritation of the skin around the stoma. Your doctor, your nurse, or an enterostomal therapist can teach you how to clean the area and prevent irritation and infection. The "Rehabilitation" section has more information about how people learn to care for a stoma.
The time it takes to heal after surgery is different for each person. You may be uncomfortable for the first few days. Medicine can help control your pain. Before surgery, you should discuss the plan for pain relief with your doctor or nurse. After surgery, your doctor can adjust the plan if you need more pain relief.
It is common to feel tired or weak for a while. Also, surgery sometimes causes constipation or diarrhea. Your health care team monitors you for signs of bleeding, infection, or other problems requiring immediate treatment.
Chemotherapy
Chemotherapy uses anticancer drugs to kill cancer cells. The drugs enter the bloodstream and can affect cancer cells all over the body. Anticancer drugs are usually given through a vein, but some may be given by mouth. You may be treated in an outpatient part of the hospital, at the doctor's office, or at home. Rarely, a hospital stay may be needed. The side effects of chemotherapy depend mainly on the specific drugs and the dose. Your health care team can suggest ways to control many of these side effects. Most side effects usually go away after treatment ends.
Biological Therapy
Some people with colorectal cancer that has spread receive a monoclonal antibody, a type of biological therapy. The monoclonal antibodies bind to colorectal cancer cells. They interfere with cancer cell growth and the spread of cancer. People receive monoclonal antibodies through a vein at the doctor's office, hospital, or clinic. Some people receive chemotherapy at the same time.
During treatment, your health care team will watch for signs of problems. Some people get medicine to prevent a possible allergic reaction. The side effects depend mainly on the monoclonal antibody used. Side effects may include rash, fever, abdominal pain, vomiting, diarrhea, blood pressure changes, bleeding, or breathing problems. Side effects usually become milder after the first treatment.
Radiation Therapy
Radiation therapy (also called radiotherapy) uses high-energy rays to kill cancer cells. It affects cancer cells only in the treated area.
Doctors use different types of radiation therapy to treat cancer. Sometimes people receive two types:
- External radiation: The radiation comes from a machine. The most common type of machine used for radiation therapy is called a linear accelerator. Most patients go to the hospital or clinic for their treatment, generally 5 days a week for several weeks.
- Internal radiation (implant radiation or brachytherapy): The radiation comes from radioactivematerial placed in thin tubes put directly into or near the tumor. The patient stays in the hospital, and the implants generally remain in place for several days. Usually they are removed before the patient goes home.
Side effects depend mainly on the amount of radiation given and the part of your body that is treated. Radiation therapy to your abdomen and pelvis may cause nausea, vomiting, diarrhea, bloody stools, or urgent bowel movements. It also may cause urinary problems, such as being unable to stop the flow of urine from the bladder. In addition, your skin in the treated area may become red, dry, and tender. The skin near the anus is especially sensitive.
You are likely to become very tired during radiation therapy, especially in the later weeks of treatment. Resting is important, but doctors usually advise patients to try to stay as active as they can.
Treatment for Colon Cancer
Most patients with colon cancer are treated with surgery. Some people have both surgery and chemotherapy. Some with advanced disease get biological therapy.
A colostomy is seldom needed for people with colon cancer.
Although radiation therapy is rarely used to treat colon cancer, sometimes it is used to relieve pain and other symptoms.
Treatment for Rectal Cancer
For all stages of rectal cancer, surgery is the most common treatment. Some patients receive surgery, radiation therapy, and chemotherapy. Some with advanced disease get biological therapy.
Radiation therapy may be used before and after surgery. Some people have radiation therapy before surgery to shrink the tumor, and some have it after surgery to kill cancer cells that may remain in the area. People also may have radiation therapy to relieve pain and other problems caused by the cancer.


![gas-15-08-01[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_2bce403e562d13e4e28a35671344d54b.jpg)
![5[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_cc16dda8c9e2ed6270cb2bc2ad75a99f.jpg)

![gas-10-08-04[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_feebfe748a52228afefc4042a926a7af.jpg)
![gas-10-08-06[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_8be7d6eb1c8ef596d8ed0229ddd1dea8.jpg)
![gas-10-08-07[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_e4a7c15c0a4b6d57fdc748eaa08cadcb.jpg)
![gastro-1[1]](http://dravinashtank.in/wp-content/uploads/ewpt_cache/300x300_95_1_c_FFFFFF_a76ddbd5b7ed6897432f87277f65753a.jpg)
