कनकधारा स्तोत्र, धन प्राप्ति का चमत्कारी उपाय
Reading Time: 5 minutes Spread the love कनकधारा स्तोत्र, धन प्राप्ति का चमत्कारी उपाय धन की तलाश में हम सभी अपने जीवन में एक समय…
Dr AvinashTank, is a super-specialist (MCh) Laparoscopic Gastro-intestinal Surgeon,
The portal hypertension itself is difficult to treat effectively, except by treating the underlying cause (where possible) and liver transplantation (if indicated and feasible).
Portal venous pressure can be reduced by medicine (beta-blockers ± nitrates) and by using surgery (shunt procedures) to create an new joint ( anastomosis) between the portal systemic veins.
Medicine
Endoscopic Therapy
Transjugular intrahepatic portosystemic shunt (TIPS)
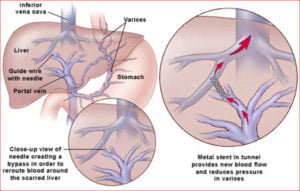
This is a radiological procedure, connecting the portal and hepatic veins using a stent. The purpose of a TIPS is to decompress the portal venous system, to prevent re-bleeding from varices or to reduce the formation of ascites. However, there are potential complications - hepatic encephalopathy and deteriorating liver function. The stent may stenose; it requires follow-up and may require repeat procedures.
Surgical porto-systemic shunts: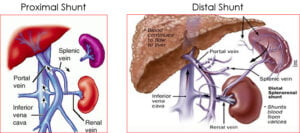
Devascularisation procedures:


Reading Time: 5 minutes Spread the love कनकधारा स्तोत्र, धन प्राप्ति का चमत्कारी उपाय धन की तलाश में हम सभी अपने जीवन में एक समय…

Reading Time: 2 minutes Spread the love Mucus Discharge from Rectum After Stoma Surgery: Normal or Concerning? If you’ve had ostomy surgery, either a loop ileostomy…
Reading Time: 2 minutes Spread the love National Doctors Day 2024: Celebrating Our Medical Heroes on 1st July. Every year on 1st July, we come together…